Doença de Peyronie: Guia Completo Sobre Causas, Sintomas e Tratamentos Avançados

Revisão Médica
Artigo escrito e revisado clinicamente pelo Dr. Alexandre Miranda (CRMRJ: 52.72103-4), Urologista (RQE: 13152) com atuação em Andrologia e pesquisador com foco internacional em Doença de Peyronie.
What is Peyronie's disease
A Peyronie's disease é uma condição fibromatosa, caracterizada por um depósito anormal de colágeno, o que gera fibrose no tecido peniano. É como se o corpo reconhecesse aquele local como necessitando de cicatrização, iniciando um processo inflamatório que, por isso, pode causar dor.
Em seguida, há uma migração de células especializadas, os fibroblastos, que começam a depositar colágeno. Esse colágeno é um material inelástico, duro e rígido, e por isso há a formação de nódulos palpáveis (a fibrose) no pênis.
Trauma é a causa principal?
Embora muitas pessoas associem a doença a um trauma ou microtrauma, apenas cerca de 10% dos pacientes relatam de fato um evento traumático como causa inicial. A verdade é que a gênese da doença de Peyronie é multifatorial.
A condição envolve fatores intrínsecos do paciente, como:
- Predisposição genética: A presença da doença de Dupuytren (contratura na mão), por exemplo, aumenta significativamente o risco.
- Fatores bioquímicos: Podem estar envolvidos radicais livres, citocinas e falha na degradação da fibrina.
- Alterações celulares: Incluindo marcadores genéticos ainda em estudo.
Diferentemente de uma cicatrização normal (onde o colágeno é reabsorvido), na doença de Peyronie o “gatilho” da cicatrização permanece ativo. Há um excesso de depósito de colágeno sem a remoção adequada, e essa fibrose impede o pênis de se distender corretamente, funcionando como uma “cola”, causando as curvaturas e deformidades.
Sinais e Sintomas: Como saber se eu tenho Peyronie?
A doença de Peyronie pode se manifestar de várias formas. Os sintomas mais comuns que um paciente pode notar são:
- Deformidades no Pênis: A curvatura é a mais frequente, sendo mais comum para cima (dorsal). Também podem surgir deformidades em “ampulheta” (estreitamento localizado) ou redução do calibre.
- Placas ou Nódulos Palpáveis: É muito comum sentir um “caroço” ou área endurecida sob a pele, resultado do acúmulo de fibrose.
- Dor Peniana: Presente em cerca de 36,7% dos casos, ocorrendo principalmente durante a ereção.
- Perda do Volume peniano: Cerca de 60% dos pacientes relatam uma perda no volume peniano.
- Perda do Comprimento peniano: Cerca de 80% dos pacientes relatam uma perda no comprimento peniano entre 1,5 a 2,0 cm. (média)
- Disfunção Erétil (Impotência): Dificuldade em ter ou manter a rigidez, presente em 20% a 50% dos pacientes.
Como é Feito o Diagnóstico Correto?
O diagnóstico da doença de Peyronie é essencialmente clínico, baseado na história relatada pelo paciente e no exame físico realizado por um urologista experiente. Durante o exame, com o pênis sob tração manual, é possível palpar as áreas de fibrose (placas) e avaliar suas dimensões.
O teste de ereção fármaco-induzida
Em pacientes com curvaturas significativas ou que relatam piora da rigidez, o exame mais útil é o teste de ereção fármaco-induzida. Esse teste permite ao especialista avaliar com precisão:
- A magnitude da curvatura.
- O padrão da deformidade (se é simples ou complexa).
- E o mais importante: a rigidez axial, que é o parâmetro mais relevante para definir o tratamento.
🎥 Assista a um vídeo e entenda como funciona o Teste de Ereção Fármaco-Induzido
Nota do especialista: E o ultrassom doppler peniano ?
Muitos pacientes perguntam sobre o ultrassom com doppler. Embora ele possa ser associado ao teste de ereção, ele não é essencial. Sua realização não modifica a conduta ou o prognóstico e, por isso, é considerado dispensável na maioria dos casos.
Métodos complementares na avaliação
Para auxiliar no diagnóstico e planejamento, outros dois recursos são importantes:
- Autofotografias: O uso de fotos do pênis em ereção, tiradas pelo próprio paciente em ângulos padronizados (conhecido como fotos de Kelami), é um recurso muito valioso e não invasivo.
- Erection Hardness Score (EHS): Quando há suspeita de disfunção erétil associada, utilizamos esta escala objetiva que classifica a rigidez peniana.
As Fases da Doença: Ativa vs. Estável
Fase Ativa (Inflamatória)
- Pain (especialmente durante a ereção).
- Piora gradual da deformidade e da curvatura.
- Possível crescimento das placas de fibrose.
Fase Estável (Crônica)
Após o período inflamatório, a doença costuma entrar na fase estável, na qual os sintomas cessam sua progressão. Considera-se que o paciente atingiu esta fase quando permanece por mais de 3 meses sem dor e sem piora da deformidade or aumento do tamanho da placa. É importante notar que, em alguns casos (cerca de 12% dos pacientes), pode ocorrer uma remissão espontânea da doença.
Opções de Tratamento para Doença de Peyronie
O tratamento da doença de Peyronie pode ser considerado desde a fase aguda (ativa), especialmente quando há dor ou perda de rigidez. A decisão é avaliada a partir dos sintomas e do impacto funcional — com ênfase na rigidez medida no teste de ereção fármaco-induzida.
De forma geral, os tratamentos são divididos em duas categorias principais:
- Nonsurgical treatments
- Tratamentos cirúrgicos

Tratamentos NÃO cirúrgicos
A seguir, abordaremos as opções não cirúrgicas, suas evidências científicas e seus reais benefícios.
Tração Peniana
A tração peniana é uma das principais modalidades conservadoras, com evidência científica estabelecida. Aproximadamente 1/3 dos pacientes apresentam boa resposta, enquanto cerca de 24% não apresentam qualquer melhoria. O uso deve ser diário, por pelo menos 3 meses. Em média, observa-se uma recuperação de 1,0 a 1,8 cm em comprimento peniano.
Onda de choque de baixa intensidade focal
As ondas de choque de baixa intensidade focais são uma opção importante, especialmente na fase aguda. Seus principais benefícios comprovados são:
- Redução da dor durante a ereção.
- Estabilização da progressão da doença (evitar progredir a curvatura).
- Melhora da função erétil
- Melhora na qualidade de vida do paciente.
É importante notar que as ondas de choque não corrigem curvaturas já estabelecidas.
Terapias injetáveis (injeção de enzima específica)
A principal terapia injetável é a injeção de uma enzimas específica que “corrói” o colágeno. Estudos mostram uma melhora média de 34,4% na curvatura. No entanto, é crucial notar que:
- O uso de placebo (injeção de soro fisiológico) já promove, em média, 18,2% de melhora.
- Portanto, o benefício adicional real da enzima é de aproximadamente 16,2%.
- Seu custo é elevado (estimado entre US$ 28.000 e US$ 36.000) e não está disponível no Brasil.
- Pode causar complicações relevantes, como hematomas, dor intensa e até ruptura da túnica albugínea.
Outros tratamentos (sem comprovação científica)
É fundamental que o paciente tenha cautela com tratamentos sem comprovação científica clara.
- Medicações Orais: Não corrigem a curvatura. A t⟑d⟑l⟑fil⟑ pode ser usada na fase aguda para tentar reduzir o depósito de colágeno, mas não reverte a deformidade.
- Cremes, pomadas e i0nt0for℮s℮: Sem eficácia comprovada.
- Oz0ni0t℮r⟑pi⟑: Sem evidência científica para tratamento da Doença de Peyronie.
Tratamentos cirúrgicos para a doença de Peyronie
As indicações para tratamento cirúrgico ocorrem quando a deformidade peniana dificulta ou impede a relação sexual, ou quando o impacto psicológico é significativo. De forma clássica, a cirurgia é recomendada apenas quando a doença está na fase estável (há ao menos 6 meses sem dor ou progressão).
Uma exceção importante são os casos com indicação clara de implante de prótese peniana por disfunção erétil significativa. Nesses pacientes, não é obrigatório aguardar a estabilização completa da doença.
Avaliação inicial: Como escolher a cirurgia correta?
O primeiro passo é avaliar a função erétil do paciente:
- Se a função erétil está preservada, opta-se por cirurgias que corrigem a curvatura (plicatura or enxerto).
- Se há disfunção erétil, a indicação clássica é o implante de prótese peniana, que resolve a rigidez e a curvatura em um único procedimento.
Plicatura (para curvaturas menores que 60°)
Esta técnica é indicada para pacientes com boa função erétil, curvaturas menores que 60° e pênis com comprimento acima da média. A cirurgia consiste em encurtar o lado “longo” do pênis (o lado oposto à placa) para igualá-lo ao lado curto, retificando a curvatura.
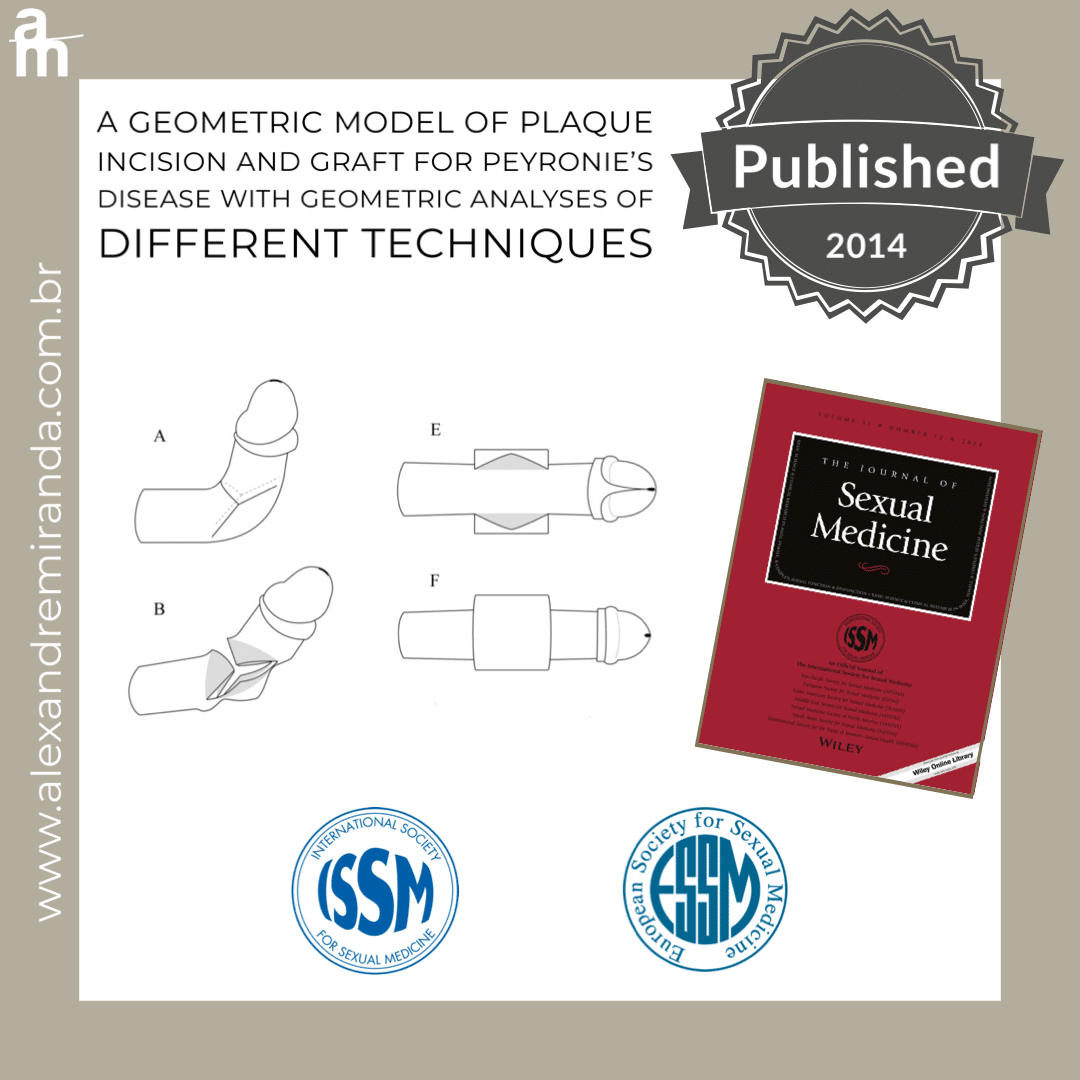
Enxerto / grafting (para curvaturas acima de 60°)
Esta é a técnica de escolha para pacientes com boa função erétil, mas com curvaturas acima de 60°, deformidades complexas (como ampulheta) ou pênis com comprimento abaixo da média. Nessa técnica, realiza-se uma incisão na placa (no lado “curto”) para expandir o pênis, e um enxerto é usado para cobrir o defeito criado.
Implante de prótese peniana
O implante de prótese é a solução para pacientes com disfunção erétil associada. No entanto, ele também pode ser indicado, mesmo em pacientes com função erétil preservada, nos casos de:
- Deformidades muito complexas (multiplanares, ampulheta severa).
- Perda importante de volumetria or length peniano.
- Queixa estética ou funcional com grande impacto psicológico.

Inovação e Liderança: Minhas Técnicas para a cirurgia de Peyronie
Embora as técnicas cirúrgicas padrão (Plicatura, Enxerto e Prótese) sejam eficazes, elas podem apresentar limitações, como risco de perda de tamanho ou disfunção erétil pós-operatória
iGrafter: Precisão Computadorizada na Cirurgia de Enxerto
A cirurgia de enxerto (grafting) é ideal para curvaturas complexas, mas o tamanho do enxerto é um fator crítico: enxertos grandes aumentam o risco de disfunção erétil pós-operatória
The iGrafter calcula a distribuição ideal das incisões ao longo da curvatura, permitindo a correção completa com uma redução de aproximadamente 50% na área total do enxerto comparado a técnicas tradicionais como o Double-Y
Resultados a Longo Prazo: Nossos estudos de acompanhamento a longo prazo (média de 111 meses) confirmam que a técnica assistida pelo iGrafter® preserva a função erétil (sem declínio significativo no IIEF-5, p=0.446), mantém o comprimento peniano e resulta em alta satisfação do paciente (81%) (resultados apresentados no Congresso Mundial da ISSM e publicados no J Sex Med, 2024)
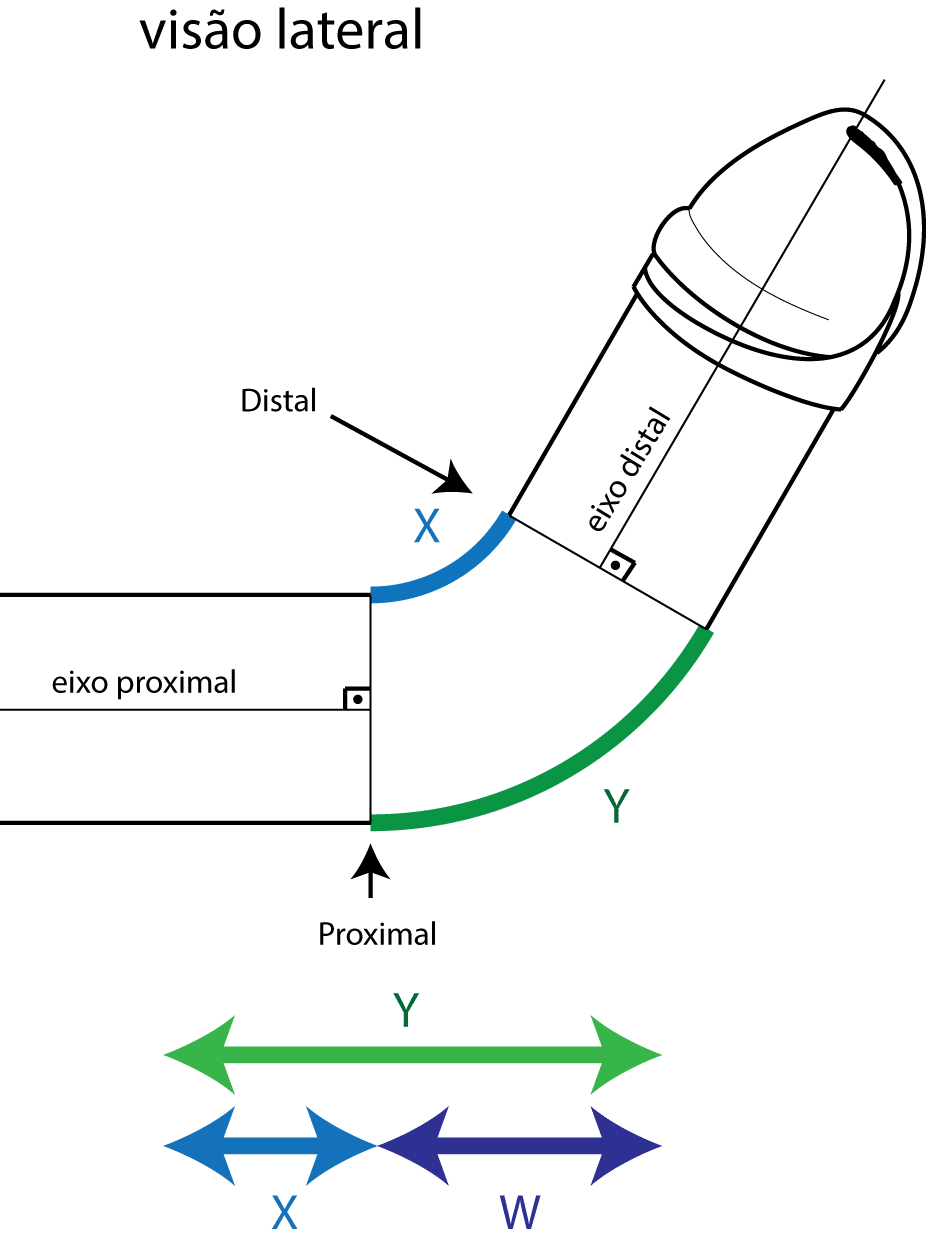
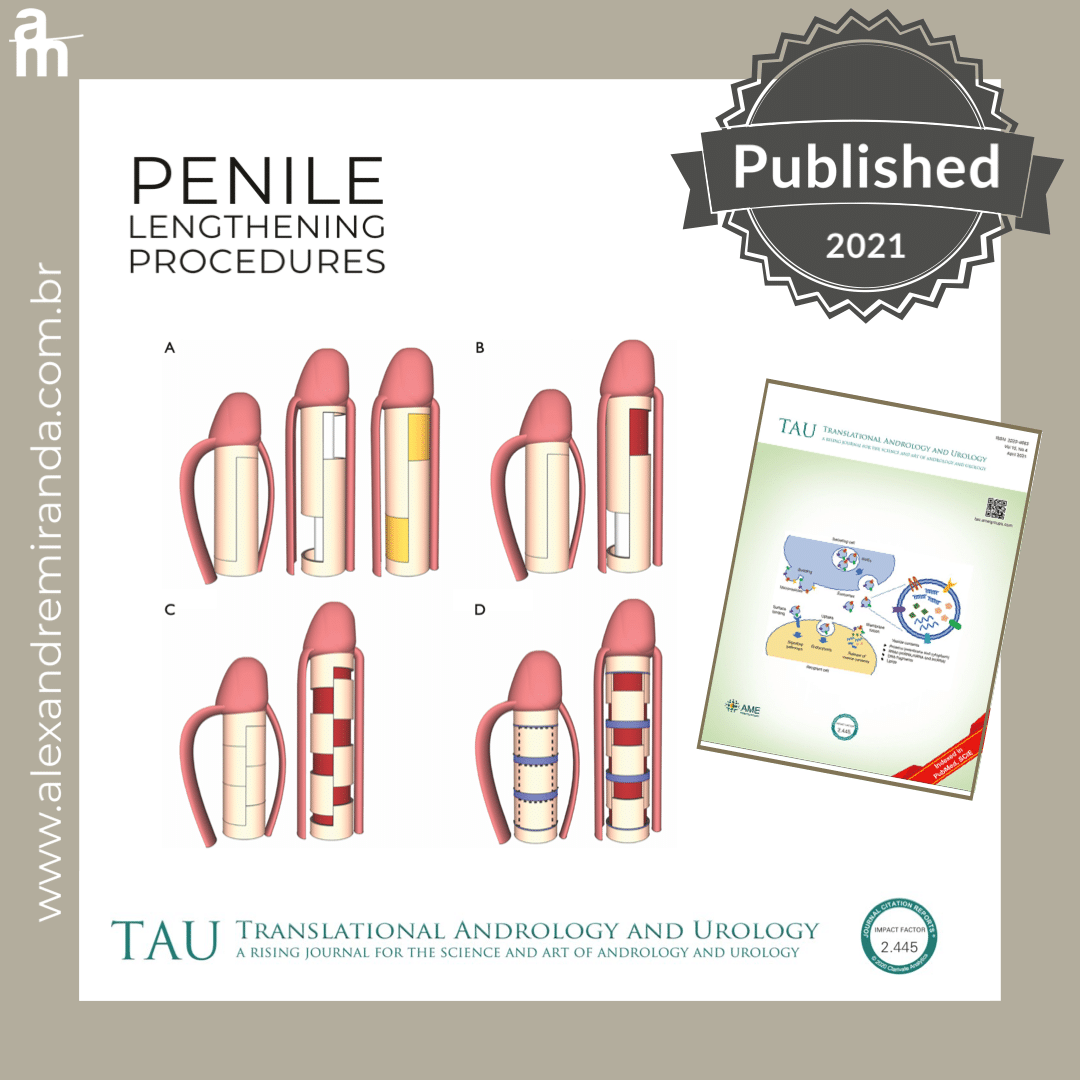
Técnica Auxética: Recuperação de Volume SEM Enxerto (Inovação Premiada)
Para pacientes com perda significativa de comprimento e calibre peniano (comum em Peyronie, pós-prostatectomia ou fibrose pós-priapismo) que necessitam de prótese peniana, desenvolvi a Técnica Auxética.
Inspirada em materiais com propriedades de expansão bidimensional (auxéticos), criei um padrão de microincisões na túnica albugínea que permite que o tecido peniano se expanda tanto em comprimento quanto em calibre, simultaneamente, sem a necessidade de enxertos
Resultados e Reconhecimento Internacional:
- Recuperação Volumétrica: A técnica demonstrou um ganho médio de 40% na volumetria peniana, restaurando comprimento e calibre perdidos. Em nossa série de casos, o ganho médio de comprimento foi de 1.8 cm e de calibre 1.2 cm
.
- Correção Completa: A expansão permite a correção de qualquer deformidade (curvatura, ampulheta) durante o implante da prótese
.
- Publicações: A base teórica e os resultados clínicos foram publicados no The Journal of Sexual Medicine e apresentados nos principais congressos mundiais, como da AUA (American Urological Association) e ISSM (International Society for Sexual Medicine)
.
- Prêmio Internacional: A técnica recebeu o prêmio de Melhor Vídeo (Best Video Award) no Congresso Anual da AUA em 2025 (Las Vegas), sendo realizada pela equipe do Men’s Health da Cleveland Clinic
.
Perguntas Frequentes sobre a Doença de Peyronie.
1. O que é a doença de Peyronie e como ela começa?
A doença de Peyronie é uma condição que provoca curvatura no pênis. Ela é causada por uma fibrose (uma cicatriz interna) na túnica albugínea, que leva a um acúmulo endurecido de colágeno.
Esse colágeno reduz a elasticidade de um dos lados do pênis. Durante a ereção, o lado oposto (saudável) distende normalmente, enquanto o lado afetado não, o que gera a curvatura.
A causa exata ainda é desconhecida (idiopática), mas sabe-se que fatores como microtraumas (durante relações sexuais, por exemplo), processos inflamatórios e predisposição genética podem contribuir para o início da doença. Apenas cerca de 10% dos pacientes relatam um trauma claro associado ao início.
2. A doença de Peyronie tem cura ou pode desaparecer sozinha?
A regressão espontânea (desaparecer sozinha) é rara, acontecendo em apenas cerca de 12% dos pacientes, geralmente na fase inicial da doença. Na grande maioria dos casos, a curvatura permanece estável ou piora com o tempo.
Quanto à “cura”, é importante diferenciar os tipos de tratamento:
- Tratamentos não cirúrguticos:Opções como injeções de enzimas específicas ou a terapia de tração penianapodem reduzir parcialmente a curvatura (em torno de 20% a 30%, dependendo do caso), mas não a eliminam por completo.
- Tratamento cirúrgico:A cirurgia é considerada a única forma de correção completa e definitiva da deformidade, seja ela uma curvatura, um estreitamento em “ampulheta” ou uma perda de comprimento associada.
3. Quais são os principais sinais e sintomas da doença de Peyronie?
Os sintomas e sinais variam de acordo com a fase da doença, mas os mais comuns incluem:
- Placa palpável:Muitos homens notam um nódulo ou área endurecida (a placa de fibrose) diretamente sob a pele do pênis.
- Curvatura do pênis:É o sinal mais conhecido. A curvatura ocorre durante a ereção e pode ser dorsal (para cima), lateral (para os lados) ou ventral (para baixo).
- Alterações na forma:Podem ocorrer estreitamentos que dão ao pênis uma aparência de “ampulheta”, além de perda de calibre ou irregularidades no contorno.
- Redução do tamanho:Até 60% dos homens podem perceber um encurtamento peniano ou redução no volume ao longo da evolução da doença.
- Dor durante a ereção:Relatada por aproximadamente 36% dos pacientes, sendo um sintoma mais comum na fase inicial (inflamatória).
- Disfunção erétil:A dificuldade de manter a ereção pode estar presente em 20% a 50% dos casos.
4. O que causa a doença de Peyronie? É trauma durante a relação sexual?
A causa exata da doença de Peyronie ainda é considerada multifatorial, ou seja, não há um único culpado.
O que sabemos é que a doença começa como uma tentativa anormal de cicatrização em uma área específica da túnica albugínea (a camada de tecido que envolve o pênis). Nesse processo, há uma ativação de células (fibroblastos) que causam um depósito excessivo de colágeno. Esse colágeno é rígido e impede que aquela região se expanda durante a ereção, causando a curvatura.
Então, não é causada por trauma sexual?
Embora muitas pessoas associem o início da doença a um evento específico, um trauma sexual claro só é identificado em cerca de 10% dos casos.
Acredita-se que outros fatores sejam mais relevantes para “disparar” esse processo de cicatrização anormal, como:
- Predisposição Genética:(Por exemplo, associação com a Doença de Dupuytren).
- Fatores Inflamatóriose estresse oxidativo.
Idade e alterações do tecido conjuntivo.
5. Como saber se estou na fase aguda ou crônica da doença de Peyronie?
A doença de Peyronie tem duas fases distintas. Saber em qual delas o paciente está é fundamental, pois isso define a estratégia de tratamento.
Fase Aguda (Inflamatória)
Esta é a fase inicial e ativa da doença. Ela é caracterizada pela progressão dos sintomas. Os sintomas mais comuns nesta fase incluem:
- Dor peniana: É o sintoma inflamatório mais comum. A dor ocorre principalmente durante a ereção, mas também pode ser sentida com o pênis flácido.
- Piora da curvatura: A deformidade continua aumentando ao longo de semanas ou meses.
- Mudanças na placa: O nódulo palpável pode parecer estar crescendo ou mudando.
- Alterações perceptíveis no formato ou calibre do pênis (como o aspecto em “ampulheta”).
Fase Crônica (Estável)
A doença entra na fase crônica quando o processo inflamatório cessa e a deformidade para de evoluir. Ela é definida pela estabilidade completa de todos os sintomas e deformidades.
Considera-se crônica quando o paciente relata o seguinte por, no mínimo, 3 meses (idealmente 6 meses):
- Ausência de dor (seja em ereção ou flacidez).
- Estabilidade da deformidade: A curvatura, o calibre (estreitamento) e o aspecto em “ampulheta”, caso existam, não apresentam nenhuma piora.
- Estabilidade da placa: O nódulo não aumenta de tamanho.
É somente após a doença estabilizar (entrar na fase crônica) que os tratamentos cirúrgicos, podem ser indicados.
6. A curvatura peniana causada pela doença de Peyronie piora com o tempo?
Sim, mas apenas durante a fase aguda da doença. A progressão não é, necessariamente, contínua por toda a vida.
- Durante a Fase Aguda: Nesta etapa, o processo inflamatório ainda está ativo. A curvatura pode piorar progressivamente ao longo de semanas ou meses, juntamente com outros sintomas.
- Ao entrar na Fase Crônica:Não. Quando a doença se estabiliza (o paciente fica de 3 a 6 meses sem dor ou piora), a deformidade costuma se manter fixa e não progride mais.
A reativação da doença após ela ter entrado na fase estável é possível, mas é considerada rara.
7. A doença de Peyronie causa impotência ou dificuldade de manter ereção?
Sim. A doença de Peyronie pode levar à disfunção erétil (dificuldade de manter a ereção) em cerca de 20% a 50% dos pacientes.
A presença de curvatura e disfunção erétil simultâneas é um dos principais motivos que levam o paciente a procurar tratamento especializado.
Isso pode ocorrer por diferentes razões:
- Dor:Na fase aguda, a dor durante a ereção pode inibir o paciente, dificultando a manutenção da rigidez.
- Dificuldade na Penetração:A própria deformidade física pode impedir o ato sexual, gerando ansiedade e perda da ereção.
- Alterações Estruturais e Biomecânicas (Instabilidade):Este é um fator muito importante. A fibrose altera a geometria do pênis, criando “pontos fracos” que comprometem a rigidez axial (a capacidade de se manter reto e firme para a penetração):
- Em casos de Estreitamento (Ampulheta):O pênis perde sustentação estrutural naquele ponto. Durante a penetração, ele pode “dobrar” ou “colapsar” nessa área mais fina, mesmo que o resto esteja rígido.
- Em casos de Curvatura:Ao tentar a penetração, a força é concentrada no lado interno (côncavo) da curva. Esse lado “afunda” ou perde a tensão, levando à perda da ereção.
- Falha Veno-Oclusiva:A própria placa de fibrose pode impedir que o pênis “aprisione” o sangue corretamente, diminuindo a rigidez geral.
O tratamento para a disfunção erétil associada ao Peyronie varia. Pode incluir medicação oral, injeções ou implante de prótese peniana.
8. Existe tratamento eficaz para a doença de Peyronie sem cirurgia?
Sim, existem tratamentos não cirúrgicos, mas é importante entender suas limitações.
Opções como a terapia de tração peniana e injeções de enzimas específicas (aplicadas diretamente na placa) podem, em alguns casos, melhorar parcialmente a deformidade.
No entanto, esses métodos geralmente não corrigem totalmente a curvatura, nem resolvem deformidades complexas (como estreitamentos em “ampulheta” ou curvaturas multiplanares).
Para uma retificação completa do pênis, especialmente em casos avançados, a cirurgia ainda é o tratamento mais eficaz e definitivo.
9. Extensor peniano ou bomba de vácuo realmente ajudam no tratamento da doença de Peyronie?
A resposta e o nível de evidência científica são muito diferentes para cada dispositivo.
- Extensor Peniano (Terapia de Tração)
O extensor peniano possui a evidência científica mais robusta para o tratamento da curvatura. Estudos mostram que, quando usado corretamente:
- Cerca de 77% dos pacientes apresentam algum grau de melhora na curvatura.
- Aproximadamente um terço (1/3) pode alcançar resultados mais expressivos.
No entanto, é importante gerenciar as expectativas: cerca de 24% dos pacientes não apresentam nenhuma melhora, mesmo com o uso adequado.
- Bomba de Vácuo
A bomba de vácuo tem evidências muito mais fracas para a correção da curvatura. A maioria dos estudos mostra uma melhora discreta ou não significativa, e não há comprovação sólida de que seu uso isolado reduza a deformidade.
Conclusão: Os extensores (terapia de tração) podem ser úteis em casos selecionados. Já a bomba de vácuo tem um papel muito limitado para este fim e não deve ser usada como tratamento isolado para a curvatura.
10. Quando é indicada a cirurgia para corrigir a doença de Peyronie?
Quando é indicada a cirurgia para corrigir a doença de Peyronie?
A cirurgia é indicada quando a doença de Peyronie está na fase crônica (estável) — ou seja, quando a curvatura parou de progredir e não há mais dor — e um dos seguintes critérios está presente:
- Dificuldade Funcional:A deformidade (curvatura, estreitamento ou encurtamento) causa dificuldade ou impossibilidade de ter uma relação sexual penetrativa.
- Impacto Psicológico:O impacto estético e emocional da deformidade afeta significativamente a autoconfiança e a qualidade de vida do paciente, mesmo que a penetração ainda seja possível.
11. A cirurgia para a doença de Peyronie faz perder tamanho do pênis ou pode recuperar comprimento?
Este é um ponto muito importante. Primeiro, é preciso entender que a própria doença de Peyronie já costuma provocar uma perda de comprimento (em média, de 2.1 a 3.2 cm). É fundamental que o paciente entenda que, independente da técnica, o pênis não voltará a ser exatamente como era antes da doença.
Efeito da cirurgia no tamanho dependerá da técnica utilizada:
- Técnica de Plicatura (Encurtamento):Esta técnica corrige a curva encurtando o lado “longo” (saudável) para igualá-lo ao lado “curto” (afetado pela doença). Portanto, esta abordagem resulta em uma redução adicional do comprimento peniano.
- Cirurgia com Enxerto (Expansão):Indicada para curvaturas mais graves (acima de 60 graus) ou deformidades complexas. O cirurgião expande o lado “curto” (o da fibrose) com um enxerto. O objetivo desta técnica é evitar a perda de tamanho que ocorreria na plicatura, preservando ao máximo o comprimento atual. Contudo, o processo de cicatrização do enxerto pode causar uma leve retração, levando a uma pequena perda de comprimento no pós-operatório.
- Cirurgia com Prótese Peniana e Expansão:Indicada para pacientes que, além da deformidade, também apresentam disfunção erétil or perdas de volume significativas. Utilizando técnicas avançadas de expansão tecidual, esta é a única abordagem que permite recuperar parte do comprimento e circunferência Estudos mostram um ganho médio de 1,9 cm de comprimento e 1,2 cm de calibre (circunferência), o que pode representar uma recuperação de até 40% do volume perdido.
12. O que é feito na cirurgia com enxerto para a doença de Peyronie e em quais casos ela é indicada?
Esta técnica é uma das mais avançadas para corrigir a deformidade preservando o comprimento peniano.
Em quais casos ela é indicada?
A cirurgia com enxerto é a opção ideal para pacientes que possuem boa função erétil (não precisam de prótese), mas apresentam:
- Curvaturas complexas ou graves, geralmente acima de 60 graus.
- Deformidades estruturais, como o estreitamento em “ampulheta” ou curvaturas multiplanares (em mais de uma direção).
O que é feito no procedimento?
O objetivo é alongar o lado “curto” do pênis, em vez de encurtar o lado “longo”. O procedimento segue estes passos:
- Planejamento por Software (O Diferencial): O planejamento preciso é essencial. Para isso, utiliza-se o iGrafter, um software cirúrgico desenvolvido pelo Dr. Alexandre Miranda e publicado em revistas científicas internacionais. Esta tecnologia calcula o formato e o tamanho exato da incisão e do enxerto necessário. A precisão do iGrafter é fundamental, pois reduz a área de enxerto em até 50% comparado às técnicas tradicionais. Isso contribui diretamente para uma melhor preservação da função erétil no pós-operatório, evitando deformidades geométricas.
- Incisão e Expansão: Com base neste planejamento preciso, são feitas as incisões na placa de fibrose (o “lado curto” da curvatura), permitindo que o tecido se expanda e o pênis se retifique.
- Posicionamento do Enxerto: O espaço criado é coberto com o enxerto (sendo o pericárdio bovino tratado um dos mais modernos, por evitar retração). Este “remendo” biológico será incorporado pelo corpo e permite que o pênis volte a distender de forma simétrica.
Esta técnica evita a perda adicional de comprimento que ocorreria na cirurgia de plicatura.
13. Quando é necessário colocar prótese peniana no tratamento da doença de Peyronie?
A prótese peniana é a solução definitiva que permite tratar dois problemas ao mesmo tempo: a curvatura e a dificuldade de ereção.
A indicação ocorre quando a doença de Peyronie está associada a um dos seguintes cenários:
- Disfunção Erétil Associada:Esta é a principal indicação. Ocorre quando o paciente apresenta disfunção erétil (presente em 20% a 50% dos casos de Peyronie) que não responde a tratamentos medicamentosos, como comprimidos ou injeções.
- Perda Significativa de Volume:Quando a doença causou um encurtamento ou afinamento (perda de calibre) severo. Nesses casos, a cirurgia com prótese pode ser associada a técnicas avançadas de expansão tecidual, sendo a única abordagem que permite recuperar parte do comprimento e calibre
- Deformidades Muito Graves ou Complexas:Em casos de curvaturas extremas, multiplanares ou grande instabilidade axial (os “pontos fracos” que fazem o pênis dobrar), nos quais as cirurgias de plicatura ou enxerto sozinhas não seriam suficientes para garantir um resultado reto e funcional.
Nota sobre o tipo de prótese: Entre os modelos disponíveis, a prótese inflável geralmente proporciona uma maior recuperação de volume, melhor resultado estético e uma sensação de ereção mais natural em comparação à prótese maleável.
14. A doença de Peyronie pode voltar depois do tratamento ou cirurgia?
A reativação da doença (recorrência) é considerada rara, especialmente se a cirurgia for realizada corretamente após o paciente atingir a fase crônica (estável).
No entanto, o risco de a curvatura voltar depende do tipo de procedimento realizado:
- Em cirurgias de Plicatura ou Enxerto:Sim, a chance de recorrência existe, embora seja incomum. O risco é maior se a cirurgia for realizada indevidamente enquanto a doença ainda está na fase aguda (inflamatória).
- Em cirurgias com Prótese Peniana:A recidiva da curvatura é praticamente impossível. A prótese atua como um suporte interno que força o pênis a ficar reto durante a ereção, impedindo mecanicamente que uma nova deformidade ocorra.
Segunda Opinião em Doença de Peyronie
A Doença de Peyronie apresenta grande variabilidade clínica e exige uma avaliação cuidadosa antes de qualquer decisão terapêutica, especialmente quando existe indicação cirúrgica. Diferenças sutis no tipo de curvatura, na presença de deformidades complexas, na rigidez peniana e no histórico do paciente podem modificar completamente a conduta.
Ao longo dos anos, muitos pacientes procuram uma segunda opinião especializada após receberem orientações divergentes ou propostas cirúrgicas com impacto potencial sobre o comprimento, a função erétil ou a necessidade futura de prótese peniana.
The Dr. Alexandre Miranda atua como pesquisador em técnicas cirúrgicas para a Doença de Peyronie, com publicações científicas, desenvolvimento de novas abordagens de enxertia, técnicas de expansão tecidual associadas ao implante de prótese peniana e participação ativa em fóruns científicos internacionais. Essa experiência permite uma análise criteriosa e individualizada, baseada não apenas em protocolos gerais, mas também em evidências anatômicas e funcionais específicas de cada caso.
A consulta de segunda opinião tem como objetivos:
- Revisar o diagnóstico e o estágio da doença
- Avaliar com precisão o tipo de curvatura e eventuais deformidades associadas
- Discutir riscos reais de encurtamento, disfunção erétil ou necessidade de prótese
- Confirmar se a indicação cirúrgica é adequada ou se existem alternativas
- Definir o momento correto para intervir, quando a cirurgia é considerada
Buscar uma segunda opinião não significa desautorizar condutas anteriores, mas sim tomar uma decisão mais segura e informada, especialmente em uma condição em que a cirurgia é irreversível e deve ser cuidadosamente planejada.
Se você já recebeu uma proposta de tratamento ou cirurgia para Doença de Peyronie e deseja uma avaliação técnica aprofundada, a consulta de segunda opinião pode ajudar a esclarecer dúvidas, alinhar expectativas e escolher o caminho mais adequado para o seu caso.
International articles published by Dr. Alexandre Miranda

New surgical technique for restoring penile length and girth
In December 2021, Dr. Alexandre Miranda published a new concept for correcting penile curvatures/hourglass deformity. This new technique is designed to restore the lost length and girth of the penis.
International Award
In 2025, the Men's Health of Cleveland Clinic received an award from the American Urological Association (AUA) at the Annual Meeting in Las Vegasusing the auxetic technique developed by Dr. Alexandre Miranda, for correction of Peyronie's disease with implantation of a penile prosthesis.
Advantages of using iGrafter
A new international article has been published demonstrating a 50% reduction in graft area and fewer errors in penile curvature corrections, utilizing the iGrafter - an APP created by Dr. Alexandre Miranda.
The potential result is better preservation of erectile function
iGrafter - Penile curvature correction application
Dr. Alexandre Miranda has developed a new surgical technique to correct penile curvatures, which has been published in the Sexual Medicine.

First 3D printed Peyronie's disease simulator
Dr. Alexandre Miranda has developed and validated a 3D-printed model for training surgeons in the correction of penile curvature.
Their work was published in Sexual Medicine
Penile enlargement during penile prosthesis implantation.
An international review article on penile enlargement during penile implantation has been co-authored by Dr. Alexandre Miranda, along with doctors from the universities of Rochester, Arkansas, and Michigan in the USA.
Issues caused by standard surgical methods for Peyronie's disease correction.
Dr. Alexandre Miranda has recently published an article in The Journal of Sexual Medicine, a prestigious international journal, discussing corrective surgical procedures for penile curvatures.
Psychological impact of Peyronie's disease - Watch the interview with psychologist Antônio Carvalho.
International Event Organized by Dr. Alexandre Miranda on Penile Curvature

25TH World Meeting on Sexual Medicine 2024
Dr. Alexandre Miranda presented, at the World Congress of Sexual Medicine, the long-term results of his surgical techniques for penile curvature correction.

Summit on Penile Curvature Surgery - 2024
Dr. Alexandre Miranda organized the first international meeting of the leading surgeons dedicated to the treatment of penile curvature.

American Congress of Urology 2022
Dr. Alexandre Miranda presented a case series using his new Auxetic surgical technique in New Orleans - USA.

Brazilian National Academy of Medicine (BNAM)
Dr. Alexandre Miranda talks about Peyronie at BNAM's Urogenital Reconstructive Surgery Symposium

Presentation at the XXXVII Brazilian Congress of Urology
Dr. Alexandre presents his new surgical techniques for Peyronie's disease


Peyronie's disease course
Dr. Alexandre Miranda teaches his technique for Peyronie's correction in a course at HCFMUSP
Penile curvature / Peyronie's disease
Watch Dr. Alexandre Miranda's interview on penile curvatures, Peyronie's disease and genital surgeries.
Presentation at the American Congress of Urology - 2016
Dr. Alexandre Miranda presented his new surgical technique for correcting penile curvature at the annual congress of the American Urological Association in San Diego - 2016.

Video publication
New video of the Dr. Alexandre Miranda Published a video at Video Journal of Prosthetic Urology of International Society for Sexual Medicine
VEJA Magazine 2019

